Nigeria’s health system is on a path of growth and keeps evolving. Information about the country’s health system is fragmented, which has occasioned the need for rapid harmonization led by the African Health Observatory Platform (AHOP). The Country Health System and Services Profile (CHSSP) will provide an in-depth description and analysis of Nigeria’s health system and services. It is likewise being conducted in Rwanda, Senegal, Kenya, and Ethiopia, which will provide the basis for comparing the health system and services’ performance across these five countries. The CHSSP is designed to be a key reference document for a wide audience including country-level policy-makers, technical staff, researchers, and development partners. They are intended to provide relevant country-specific and comparative information to support policymaking, analysis, and implementation of approaches related to the re-engineering of health systems and services in the African region.
To commence documenting Nigeria’s CHSSP, the Health Policy Research Group (HPRG), University of Nigeria, which hosts the Nigerian National Centre of AHOP conducted its kickoff meeting to prepare authors for the task ahead. The meeting took place at Hotel Sylvia, Enugu, from 13th – 15th June 2022. Partners with the HPRG on the CHSSP project were in attendance, and they include Veritas University, Association of Public Health Physicians of Nigeria (APHPN), Nigeria Institute of Medical Research (NIMR), Federal Ministry of Health, Nigeria (FMoH), and a representative of the World Health Organisation.
Nigeria’s CHSSP Authors
During the meeting, Dr. Enyi Etiaba who is the Project Manager of AHOP in Nigeria emphasized the overall goals of AHOP in the directions of knowledge synthesis and evidence translation, as she stated that the CHSSP is one of the outputs of the stated goals. She used this opportunity to ensure that all CHSSP authors are aligned with the ideals of AHOP, even as they work on the CHSSP project.
Dr Enyi Etiaba introducing AHOP and CHSSP
Documenting the CHSSP will need a uniform reference manager. The gathering was an opportunity for all authors to run through the endnote reference manager, as the approved reference manager for CHSSP documentation. Facilitated by Dr Chinyere Mbachu, authors successfully downloaded the endnote reference manager, went through step-by-step process of uploading reference materials and sources into it, and could make citations as they write. Authors are expected to make use of the Harvard Referencing Style throughout their writing.
Dr Chinyere Mbachu facilitating a session on Endnote reference manager
In addition to the above, CHSSP authors were introduced to the AHOP writing style by Dr Enyi Etiaba. Important points to note include the use of British style (e.g., use organisation instead of organization), dates should be written without punctuation signs, large figures should be written using spaces as against commas, health care should be written as “health care” and not “healthcare”, hyphenate “evidence-based” when used as an adjective but write without the hyphen when used as a noun, etc. Click here to download AHOP writing style guide.
At about noon time, authors had a virtual meeting with the CHSSP Editors from the London School of Economics (LSE) and WHO-African Region (WHO-AFRO). Concerns drawn from the 11 Chapters of the CHSSP were listed and clarified. The 11 chapters comprise the overall context of Nigeria; organization and governance of the health system; health financing; health workforce; medical products and health technologies; health infrastructure and equipment; service delivery; health information and information systems; performance of the health system (outputs); health services coverage and system outcomes; conclusion and key considerations. The meeting with LSE and WHO-AFRO helped resolved grey areas. It was agreed that authors should keep in touch with the Editors as they write, and lead authors will participate in a monthly meeting with LSE and WHO-AFRO for the duration of the writing stage of the CHSSP project. Also, the overall lead author from the National Centre must go through submissions before they get to the Editors.
Cross-section of CHSSP Authors meeting virtually with LSE and WHO-AFRO
Authors agreed with the Editors on the need to concentrate on national-level data given the timeframe of production and AHOP’s concentration on secondary sources of data. To help the authors, there are some materials in the SharePoint for this project. All authors now have access to the SharePoint. It was also agreed that more time will be allotted to the completion of Chapters 9 and 10 since they are dependent on the completion of the fore chapters. Authors were reminded to concentrate more on the Excel spreadsheet for needed information than the writing template, as some information in the latter may be wrong. Click to download the slides of LSE/WHO-AFRO
According to Professor Obinna Onwujekwe who heads the HPRG and leads the AHOP Nigerian National Centre, the CHSSP when concluded will be both means and end, in the sense that its recommendations will be used for health system strengthening towards the achievement of the health-related SDG targets, especially Universal Health Coverage (UHC) in Nigeria. As a means, it will also serve as evidence-base for the development of the 3rd National Health Sector Development Plan (NSHDP III), a resource for the planned Nigeria Health Sector Reform Programme and the national UHC plan. It will also provide the required information for the development or revision of policies and strategies in the health sector in Nigeria.
Prince Agwu commented on the dissemination of the CHSSP, which will target academia, policymakers, frontline practitioners, communities, media, and civil societies. Strategies for dissemination will keep evolving and will be cross-sectoral.
More on capacity building, CHSSP authors were taken through data sourcing strategies by Prince Agwu and Uche Ezenwaka. The use of Boolean Operators, introduction to new search engines and databases and the use of keywords were discussed extensively. Uche introduced CHSSP authors to janebiosemantics. On specific data from the Federal Ministry of Health, Martins Otuamah took CHSSP authors through specific databases that will be of help in the documentation process. And finally, on capacity building, Prof BSC Uzochukwu, an HPRG and AHOP National Centre lead took authors through academic writing and production of policy briefs. Authors were exposed to non-linear methods of academic writing and the rationale behind building quality academic arguments. This was one of the high points of the CHSSP meeting.
In all, the National Centre is looking forward to 7th July 2022 for first submissions, and 14th and 15th July 2022 for a second workshop that will focus on writing. “We are hopeful authors will stick to the timeframe, and will produce top-quality chapters, which is the signature of the HPRG. Otherwise, we may be forced to substitute authors if and when needed”, as said by the Nigerian AHOP lead, Prof Obinna Onwujekwe.
Research.com, a prominent academic platform for scientists, has just published the 2022 Edition of its Global Ranking of Top 1000 Scientists in the area of Social Sciences and Humanities. Three academics from the University of Nigeria, including the University, made the list. Professors Obinna Onwujekwe, Benjamin Uzochukwu, and Jude Ohaeri ranked 1st, 2nd, and 3rd respectively in Nigeria, and 892, 3052, and 4039 on the globe, respectively. Also, the University of Nigeria is the lone university in Nigeria that made it to the top 400 on the globe in terms of research outputs from the social sciences and humanities. The University of Nigeria is ranked 305 in the world and 1st in Nigeria.
The green entrance of the University of Nigeria
Professors Obinna Onwujekwe, Benjamin Uzochukwu, and Jude Ohaeri have long been listed as tops in several global ratings of scientists. A Google Scholar search on Professor Obinna Onwujekwe as of 9th June 2022, shows that he has 22,287 citations, 54 h-index, and 210 i10-index. While Professor Benjamin Uzochukwu has 25,025 citations, 46 h-index, and 133 i10-index. Unfortunately, we could not retrieve that of Professor Jude Ohaeri at the time of writing. Speaking to Professors Obinna and Benjamin, we can confirm that the duo are not resting or retiring any time soon from active research, especially, implementation research. They are of the view that governance and development rise on the availability and utilization of scientific evidence, and fall on the dearth and weak recognition of it.
Professor Obinna Onwujekwe
Professors Obinna Onwujekwe and Benjamin Uzochukwu run the Health Policy Research Group, University of Nigeria, which is famous for the production of cutting-edge scientific evidence. It is equally a hub for the nurturing of young scientists. Both Professors remain committed to mentorship, as they look forward to young scientists from Africa carving a niche for themselves in global science.
Professor Benjamin Uzochukwu
The ranking by Research.com is constructed using the H-index data gathered by Microsoft Academic and includes only prominent scientists with an H-index of at least 30 for scientific papers published in the field of Social Sciences and Humanities.
As quoted from the words of Imed Bouchrika for Research.com, “… this is indeed an important accomplishment for you and your university”. The Health Policy Research Group, University of Nigeria joins in congratulating its noble Professors and the University of Nigeria, as it continues in its restoration of man’s dignity!
By Shalom Obi, Osondu Ogbuoji, Wenhui Mao, Minahil Shahid, Gavin Yamey, and Obinna Onwujekwe
In the coming years, about a dozen middle-income countries are expected to transition out of development assistance for health (DAH). This is so because the eligibility criteria set by most multilateral donors are based on income per capita or rise in GDP. However, an increase in income per capita does not necessarily mean a reduction in disease burden. For example, despite an increase in GDP, Nigeria still stands out as very unprepared for the upcoming transition, based on poor health indices, very low domestic financing for health, and poor government commitment to health.
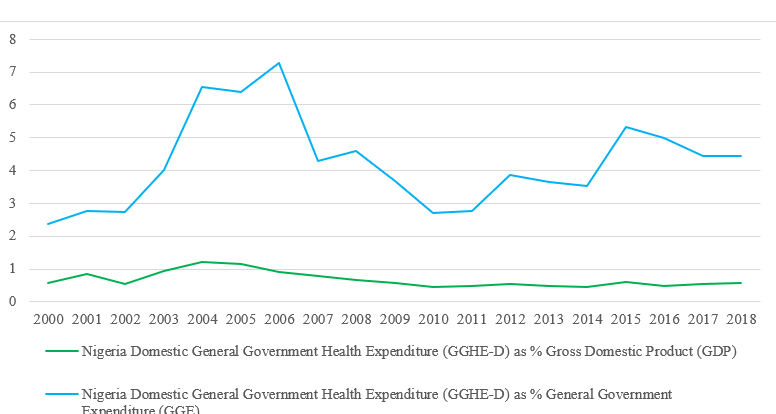
Nigeria is vulnerable to setbacks, in event of health-focused donors exiting its health funding space because the country struggles with a low per capita income, debt burden, weak capacity to efficiently use public resources, limited and less effective health systems, and weak governance and public institutions. More so, considering the low government funding for health (see Figure 1 below), the impending financial gap will most likely shift to out-of-pocket spending which constitutes 75.2% of total health expenditure. This will be catastrophic and may drive more of the vulnerable population below the poverty line. The decline in donor funding has already been reflected in suboptimal service delivery and health service users are now having to pay for previously free-of-charge services.
Figure 1: Trend of Domestic General Government Health Expenditure (GGHE-D) Global Health Expenditure Database
The more currently appropriated funds for health are not subject to high-level accountability, the effects on the vulnerable may likely to be grave, further drawing the country away from achieving UHC. With changes in DAH and impending transitions, there is an urgent need for sustainable solutions, as stakeholders must begin to think about how to fund healthcare when external funds decrease or end.
For evidence-driven transitioning, away from DAH, stakeholders may wish to refer to a qualitative research that used Vogus and Graff’s expanded framework for evaluating the readiness of Nigeria’s transition. Unfortunately, the illustrated gaps (see Figure 2) identified in the study show that Nigeria is not currently prepared to sustain donor-funded programs and make progress if/when donors leave.
Figure 2: Gaps – using Vogus and Graff’s expanded framework for evaluating country readiness for transition of donor-funded health programs to domestic ownership (Vogus and Graff, 2015)
The above framework shows clearly that Nigerian health system is mostly unprepared to transition out of DAH and make progress towards UHC. This is predominantly due to policy implementation gaps, unaccountability and corruption, and a lack of initial transition plans at the onset of health programs.
Policy implication
To overcome the challenges and bottlenecks that hinder policy implementation and close these gaps,
Policymakers should consider the feasibility, sustainability, and accountability of policy implementation during the policy process. They should ensure that there are feasible road maps for apt implementation of pro-UHC policies.
Secondly, crucial steps must be taken to ensure that transition plans are factored into program planning from the onset, and not as an addendum. A well-grounded health plan that puts transition in perspective is needed to foster sustainability and progress towards UHC at the time of transition.
Nigeria must also endeavor to make political commitment to health – at least improve from current 5% of annual budget allocated to the health sector, while racing toward the 15% commitment as promised in the Abuja declarationof 2001. This will enable the country to integrate healthcare programs and build the overall health system to transition smoothly out of various donor programs, whilst making progress towards UHC. Meeting this commitment has become even more critical given the effects of COVID-19 pandemic.
Lessons for upcoming transitioning countries
Upcoming cohort of transitioning countries should have a robust transitioning plan in place to sustain gains of donor funds and make progress toward UHC. Transition plans should not be an afterthought, but a well-incorporated aspect of health programs’ plans. Therefore, donors and recipient countries should ensure that transition plans are built into health programs at the planning stage. Furthermore, it is not enough for upcoming transitioning countries to have pro-UHC policies, they should also have roadmaps for implementation, with broad stakeholder involvement. It is also crucial for such countries to give careful consideration to increasing their fiscal space for domestic funding for health, integration of health programs, and building the overall health system. This will engender sustainability and ensure progress towards UHC at the time of transition. Donors and recipient countries should endeavor to have inbuilt transition plans to give direction to program implementation and enable institutionalization of service delivery processes for continuity.
Conclusively, to manage transitions from DAH and make progress towards UHC, the Nigerian government needs to identify and address implementation gaps, as well as systematic gaps in using domestic resources for financing critical health services. Policymakers should identify clear road maps for the implementation of the existing pro-UHC policies. Furthermore, funds should be redirected to building the overall system—consolidating and coordinating programs and linking them into the overall health system, health financing priorities, and policies. Instead of continuing to invest in parallel programs, a comprehensive and functional structure for continuity, one that will be robust enough to withstand decreasing external funds or donor exits, should be developed at the national and sub-national levels as a matter of urgency.
Shalom Obi is a Research Fellow at the Health Policy Research Group, University of Nigeria, with focus on health policy research and community health systems.
Obinna Onwujekwe is a Professor of Health Economics, Systems and Policies at the University of Nigeria Enugu Campus. He is the Chief Editor of the African Journal of Health Economics, and the Coordinator of the Health Policy Research Group, University of Nigeria. He also coordinates the African Health Observatory Platform (AHOP) for Health Systems, Nigeria Center.
Acknowledgement: We thank Dr Godstime Eigbiremolen for the review of the blog