Evidence from Cross Programmatic Efficiency Analysis of Health Programmes (CPEA) reveals that inefficiencies marr investments in Nigeria’s health sector
By Health Policy Research Group (HPRG), University of Nigeria
What to know about Cross Programmatic Efficiency Analysis of health programmes
Nigeria’s health sector enjoys investments from bilateral and multilateral agencies like the WHO, USAID, Global Fund, etc., that come as partners to strengthen the country’s health system and improve health service delivery. Investments from partners are add-ons to budgetary allocations to the health sector by federal and state governments, as well as locally sourced resources for health. Yet Nigeria’s health space is said to suffer suboptimal funding, which is a vital concern documented by the Lancet on Nigeria’s investment in health and population health outcome performance.
However, conversations are currently about how to get value for the current ‘suboptimal’ health investments. Indeed, more money may not guarantee more health, if steps are not taken to ensure efficient allocation and utilization of scarce resources in ways that offer maximal value for every penny invested in the health sector.
To address these concerns about efficiency in resource allocation and use of resources in health sectors, the WHO developed a diagnostic approach, the Cross Programmatic Efficiency Analysis (CPEA). CPEA focuses on mapping programmes within the health systems of countries, for the purpose of identifying inefficiencies. These inefficiencies manifest in the form of duplications, overlaps and misalignment of roles and functions across or within governance, procurement system, service delivery, financing, and information management systems. And they have implications on success or failure of priority health programmes, such as HIV, Tuberculosis, Malaria, Immunization, and Reproductive Maternal, Newborn, Child and Adolescent Health (RMNCAH).
CPEA study was conducted in three states in Nigeria (Anambra, Imo and Sokoto). Although there is an implementation focus in Anambra, with plans for spreading into other states in future. The study also considers the need to reflect with federal agencies like the Federal Ministry of Health (FMoH) over the work being done at state level, since most of the partners will always come into the country through the ‘Federal gate’.
Stakeholders meet to look at previous CPEA findings
The CPEA study was conducted between 2018 and 2019, using key-informant interviews and review of documents. As the study nears implementation of its key recommendations, concerned stakeholders such as directors at the FMoH, State Ministry of Health (SMoH) including commissioners of health, Executive Secretaries/Chief Executive Officers of health agencies, representatives of development/implementing partners, and health systems and health economics expert, were invited to a 2-day implementation meeting (18th and 19th April 2023) at Valencia Hotel, Abuja.
The stakeholders yet again looked through the key findings from the CPEA study, identifying areas of improvement within their health systems since 2019 when the CPEA study was concluded. Indeed, there were some remarkable improvements, especially around centrally governing diverse partners through the SMoH.
A representative of one of the states said, “Unlike at the time the CPEA study was conducted, we now have ownership of health programmes in our state, particularly in terms of approval and oversight. It is no longer the usual case of partners coming in with programmes and we have no idea of what is happening. That has changed since after 2019”.
Nevertheless, there was consensus that a number of inefficiencies still exist in the coordination of the programmes, particularly in areas of financing, information management, service delivery, and some components of governance that have to do with planning, human resource management, and sustainability of programmes at the exit of donors.
Cross-section of participants with the Director of Planning, Research, and Statistics, Federal Ministry of Health and Commissioner of Health, Sokoto State
In retrospect, what were the findings from CPEA?
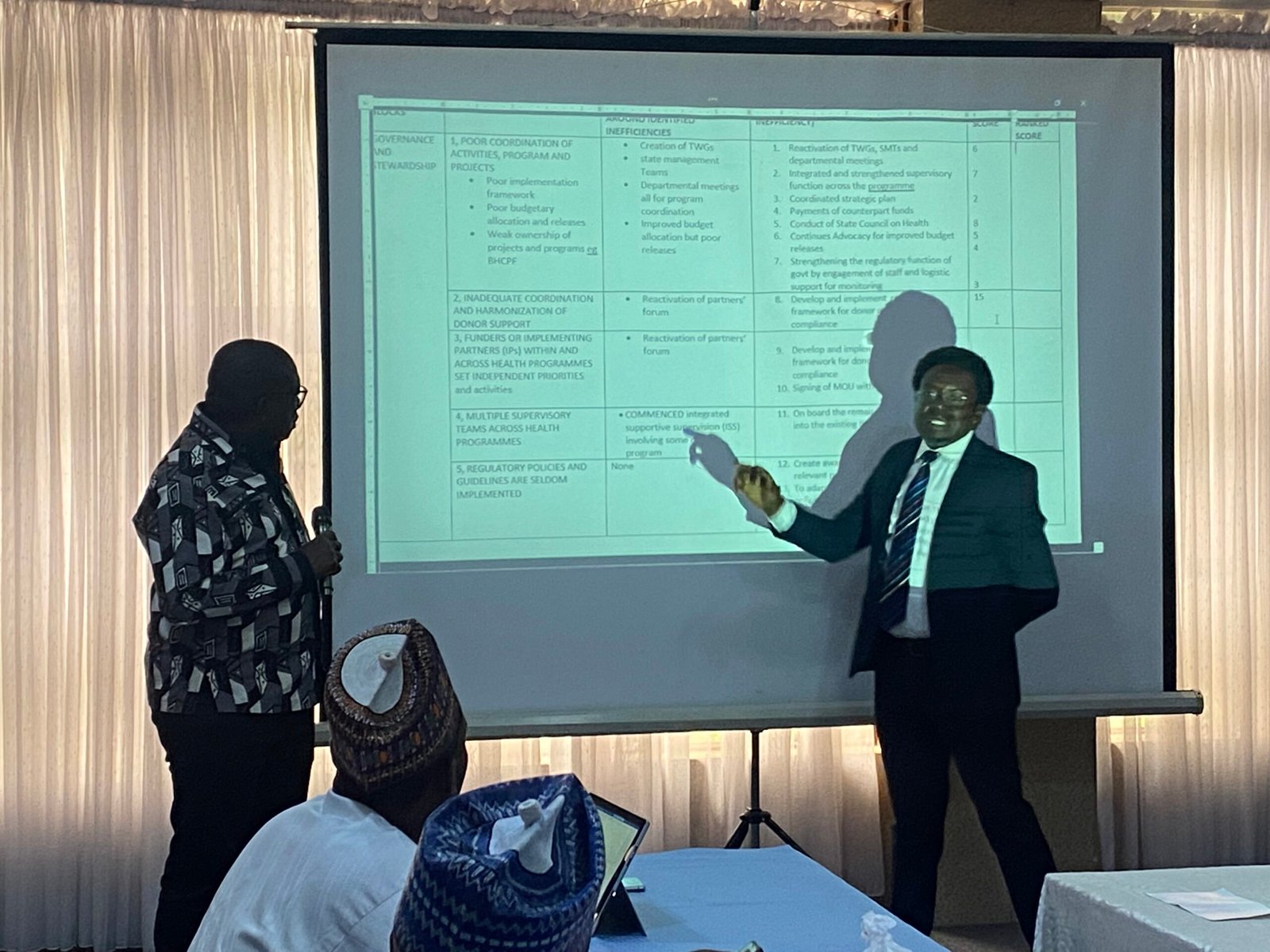
During the 2-day meeting, health systems and policy experts from the Health Policy Research Group, (HPRG) University of Nigeria, led by Professor Obinna Onwujekwe, together with Dr Francis Ukwuije of the Health Financing Technical Office of the World Health Organisation, Nigeria, recapped key findings from the CPEA study done in Anambra, Imo, and Sokoto States. Interestingly, identified inefficiencies were common across the three states. Inefficiencies were found in the following areas:
Partners pursuing financing of health programmes that do not align with the health priorities of the states.
Decisions of health programmes to execute by partners at the federal level with almost no input from the states.
Due to the lack of contributions by stakeholders at the state and local government levels to health programmes, partners could bring health programmes that are not actually needed in certain communities, which leads to wastage of resources.
Partners fund health programmes and assign budget lines that have already been captured in the national or state health budgets, leading to more wastage of scarce resources.
While there is a need for diverse health programmes, supervisory and accountability lines should be mainstreamed for efficiency. As against having too many supervisory/accountability lines, like “too many cooks, spoil the broth”.
“Too many cooks spoiling the broth” was again manifest in information management. When different programmes have unique data reporting tools and dissemination platforms, it could cause confusion and even data inaccuracy, which could affect decision-making.
Health programmes may not be informed by evidence, as gaps between generated data and decision-making persist.
Health programmes could be counterproductive to the management of human resources for health, in the sense that health workers in a bid to attend to the demands of programmes may neglect the core responsibilities of attending to patients in facilities. And some of the health workers could want to lobby themselves into health programmes with more funding.
As inefficiencies across the health programmes persist, what way forward?
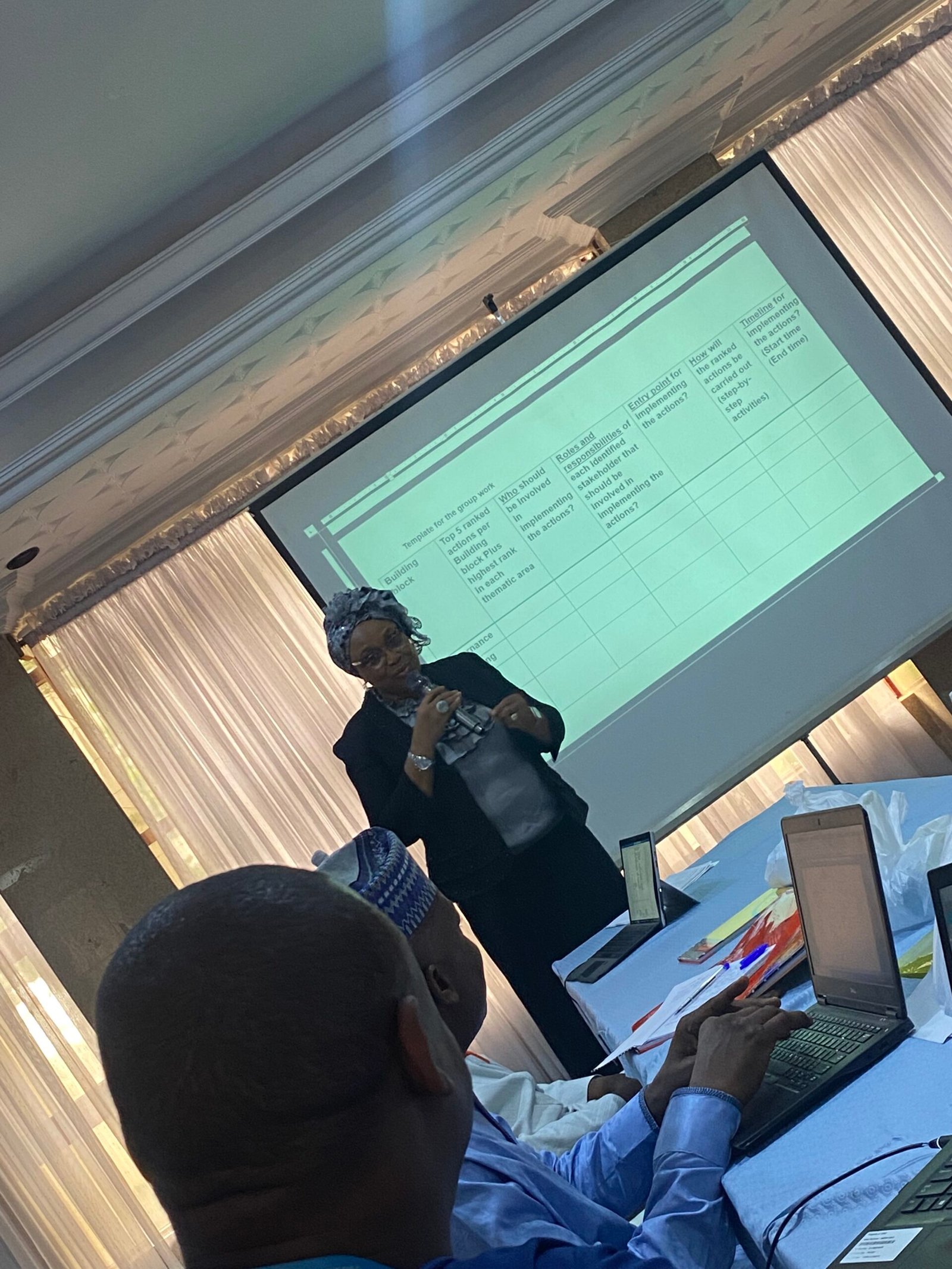
Interestingly, stakeholders acknowledge that these inefficiencies must be tackled if the health system will make progress. Uche Ezenwaka on behalf of the HPRG, led the activity on priority and agenda setting in addressing the identified inefficiencies.
First, the stakeholders were made to understand the concepts of feasibility and fidelity in designing priorities and agenda. Followed by being talked through the core focus of CPEA in areas of governance, financing, service delivery, information management, and procurement.
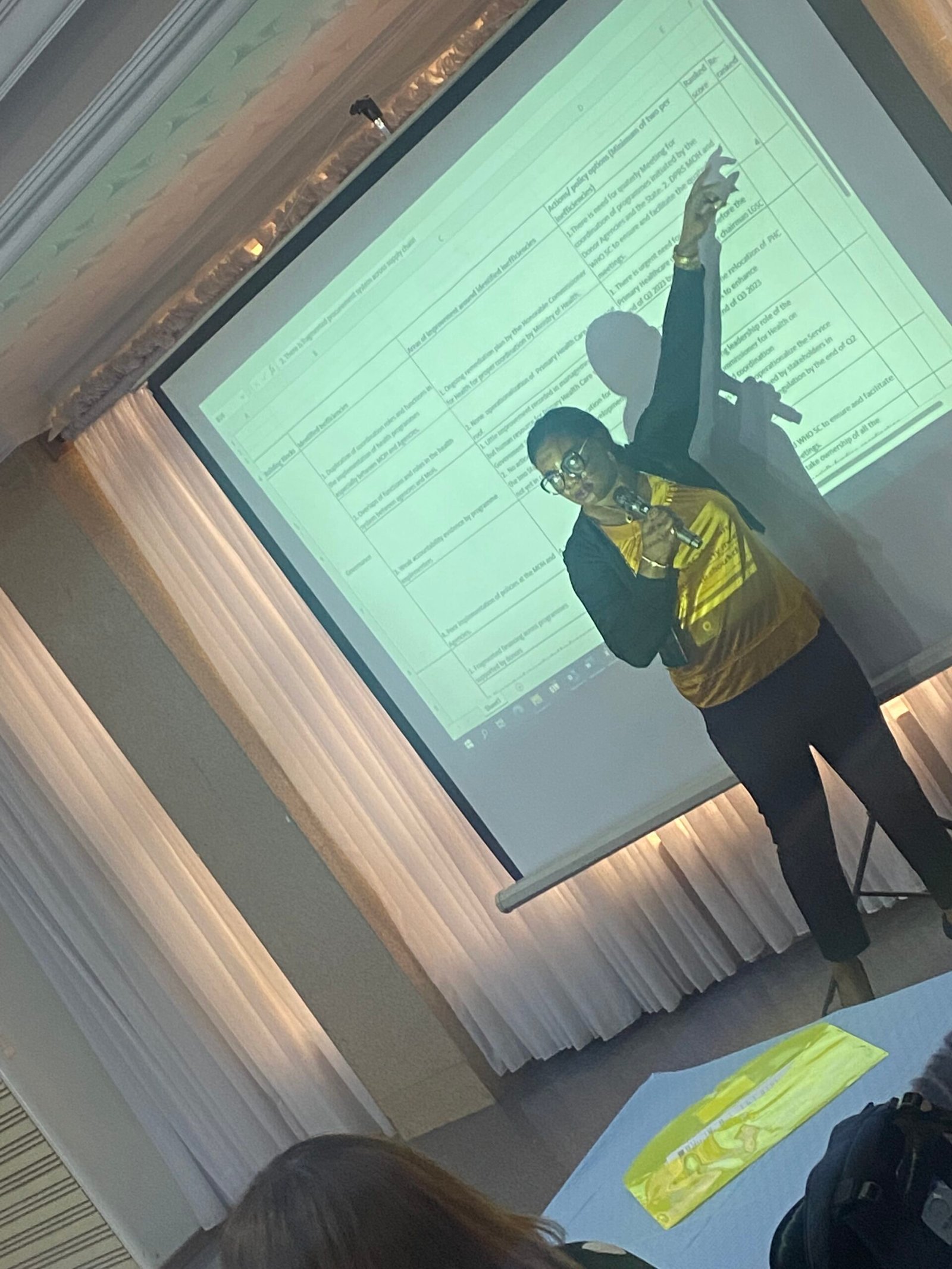
Although still a work in progress, a summary of agenda setting achieved by the states with support from the federal level, are:
Establish a special desk office under the Commissioner of Health that will compulsorily be the entry and exit of health partners supporting programmes. This will help states to assume ownership of the programmes and stay well informed of the programmes’ contents and management.
Activate the health partners coordination committee (HPCC) in the FMoH, and source funding for the committee through budgetary allocation to the Ministry. This will help achieve harmonization of programmes, as well as supervise coordinated input from states on health programmes.
Aggregate insights from facilities and local government health authorities before drawing up budgets for the health sector in states.
Advocate for early passage of annual budgets to guide annual operational plans for the health sector.
Organise state-owned partners’ forum for harmonization of health programmes in the state and achievement of health spending based on unique health priorities in states.
Establish desk offices in Ministries of Health for scouting and distilling research evidence for use by policymakers in engaging partners and members of the state executive council.
Engage and sensitize the Civil Society Groups to participate in monitoring the activities of partners and demanding accountability.
Guided by the Primary Healthcare Under One Roof (PHCUOR) to improve the relationship between the State Primary Healthcare Development Agencies and Local Government Health Authorities to strengthen supervision of programmes at the primary healthcare level.
Activate state level data operation center (DOC) that collates, harmonize and coordinate data for decision-making commissioned by UN and WHO to help streamline reporting line and data.
Establish a Logistic Management and Coordination Unit (LMCU) to address fragmented procurement system across supply chain
Establish a Health Workforce registry to serve as a database to enable acute and timely evidence-based health workforce information and management.
Conclusion
The involvement of top players in the health sector of the selected States is an important step towards the achievement of the desired efficiency across the health programmes and health sector at large. Also, the acknowledgement of inefficiencies by these top players, and the commitment of their time to begin drawing up feasible and workable remedial strategies, offers a strong sense of conviction. The implementation of CPEA is large on prioritization, implying that the implementers understand how ambitious it can be trying to address all inefficiencies. So, the focus will be on specific state priority areas for efficiency. Lessons learnt will be used to pursue CPEA in other states of the country.
Acknowledgement
(1) World Health Organisation
(2) Federal Ministry of Health, Nigeria
(3) Resource for Development (R4D)
(4) Strategic Purchasing Africa Resource Centre (SPARC)
(5) State Ministries of Health, Anambra, Imo, and Sokoto.